29th March 2018
What is this?
This page introduces readers to the the use of Peer-to-Peer SupervisoryStructures, which is critical for Working with your TEAM, one of the Core Features of AMBIT practice, and in particular this relates to the AMBIT Stance of Keyworker well-connected to wider team.A key point is that this is work that involves all the protagonists (our clients, and ourselves as workers) in anxious worrying situations.
AMBIT trainings spend some time emphasising that if this work does NOT make you worried at times, then you are probably in the wrong job, as you are out of touch with the reality of what is at stake.
Mentalization, and its fragility in situations of anxiety, is something that underpins not only much of the therapeutic work with clients, but also the relationships between members of an AMBIT team. AMBIT-influenced teams place as high a priority on attending to the mentalizing of their professional peers as they do upon stimulating and sustaining mentalizing in their clients.
AMBIT Training
The AMBIT training includes a section on Learning about Supervisory Structures.Implications
It is important to note that the kind of peer-to-peer supervision described in AMBIT is not instead of ordinary clinical Formal supervision arrangements (that Governance arrangements in the wider system will determine) but are an additional feature; defining the particular culture of Working with your TEAM that is deliberately and explicitly developed in an AMBIT-influenced service.Live, responsive, accessible supervision
The team is expected to use appropriate technology to support this (mobile phones, telephone conferencing, mobile email, etc), enabling team members to form a Reflective Quorum, flexibly, and at short notice. Seeing this as part of the daily work rather than an 'occasional extra' is central to the AMBIT model.This core feature is adopted because of the considerable potential for individual practitioners to end up working in isolation in a community setting with high risk and potentially adversarial clients. In our view, apart from impact on staff morale that such isolation can cause, clinical effectiveness and decision-making also become compromised as practitioners struggle to ‘think’ (Mentalize) in such high stress contexts.
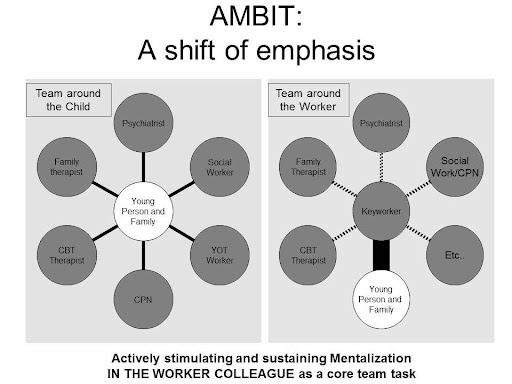
A Team around the Worker
We know that Mentalization is restored in secure relationships. Access to immediate phone or face-to-face supervision needs to be positively supported by a whole team approach, which recognises the need for such back-up as essential to such services. Doing this work for each other is seen as a CORE part of a worker's role, not an "added (optional) extra"!This is something of a shift from the traditional notion of the "team around a child" (which may still have great value, but can drive Dis-integratedInterventions), towards an arrangement that is about the "TEAM AROUND THE WORKER"
Implementing and Sustaining this peer-to-peer supervision:
Rituals and Disciplines within the team define this culture of mutual support, and an important example is the way in which such consultations are marked out and structured (see Thinking Together and Passed-outwards Discussion.)
The critical component of this process is to enable a conversation to take place between a front line practitioner who is exposed to the full multi-dimensional aspects of the young person’s difficulties and a member of the clinical team who will know the case but who is not emotionally engaged with the family members. The Ripples in a Pond analogy is used to explain this aspect of the practice. Another metaphor that we routinely use to describe this relationship is to describe the front line practitioner as a deep sea diver in which the meta-team is likened to those in the Dive Boat.
Transparency
Such supervisory input is provided in a transparent way with the family and young person so that they are aware that the front line practitioner is supported by a wider team (note one of the Core Features of AMBIT is the principle of Keyworker well-connected to wider team.
Team Meetings
The availability of this live supervision needs to be complemented by Team Meetings which provide weekly group-based Formal supervision of the clinical team. Such group supervision could be likened to an in-patient ward round in which the weekly treatment goals are reviewed, risks reassessed etc, but with particular attention to ensuring that the meeting addresses the needs of the workers who attend - which is helped by structuring Case discussion along the lines of Thinking Together conversations.
Line Management
KeyWorkers are under the line-management of a lead clinician who is responsible for ensuring that appropriate supervision is provided for each activity that he or she undertakes. A psychiatrist provides medical assessments, and is responsible for the prescribing of medication and any other physical treatment.
The MetaTeam
The Meta-team may in some situations be those KeyWorkers who are not working directly with a particular young person, but who make themselves available to the Keyworker who is "in the thick of it" via a Reflective Quorum. More formally, the MetaTeam refers to the team of specialist professionals who may not sit directly within the team, as keyworkers with caseloads themselves, but who have given consent to an agreed level of consultation to the team about areas requiring more specific expertise.
ExpertsByExperience
The team should aim to recruit over time a panel of Experts By Experience, who can be consulted on problems of managing the difficulties of young people and their families.